Welcome to Newsletter 77
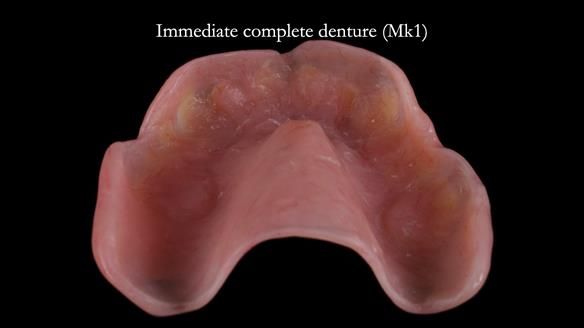
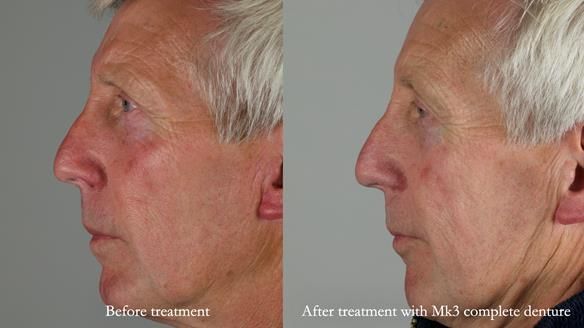
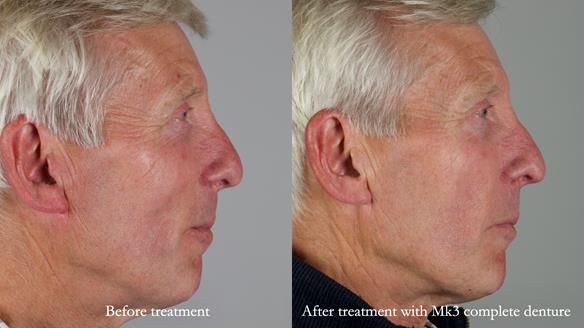
Immediate complete upper denture for Jeremy
Apologies if you receive this newsletter twice – I send it at different times so colleagues around the world can receive it conveniently. My aim is simple: to help more people make better dentures.
Prior to seeing me, Jeremy had considered dental implants and attended several consultations with different dentists, but he decided against this. He was then referred to me by a local colleague for a denture-based solution.
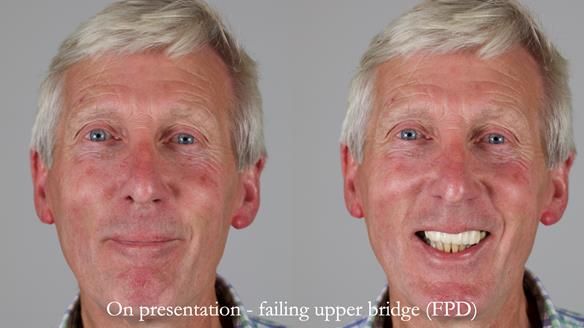
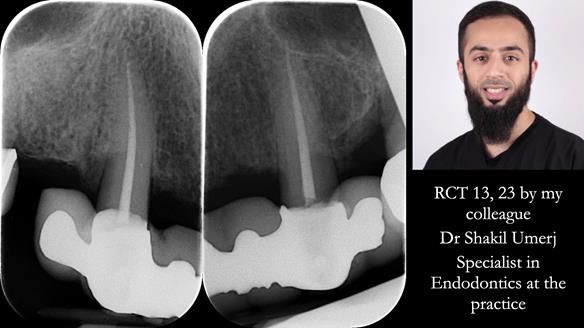
Jeremy’s upper bridge, supported by the canine teeth (13 and 23), was failing both aesthetically and functionally.
- On smiling, the bridge was clearly visible and did not look natural, as the ceramic had been ground back.
- Functionally, the bridge was unstable, due to Periodontitis – Stage IV, Grade C (generalised).
- The upper molars (UR7 and UL7) had also failed and required removal.
The original treatment plan
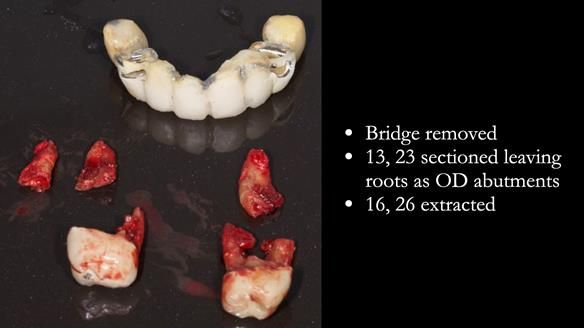
- Extract the failed molars and dismantle the bridge.
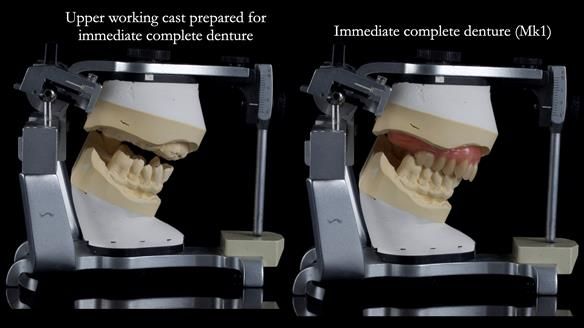
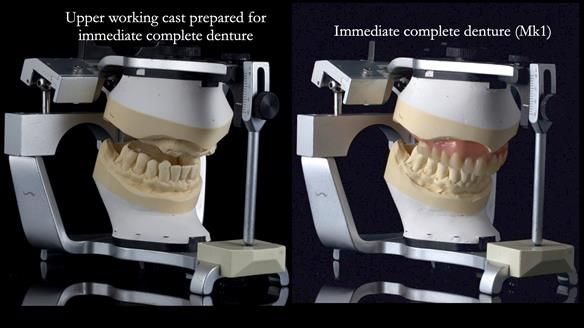
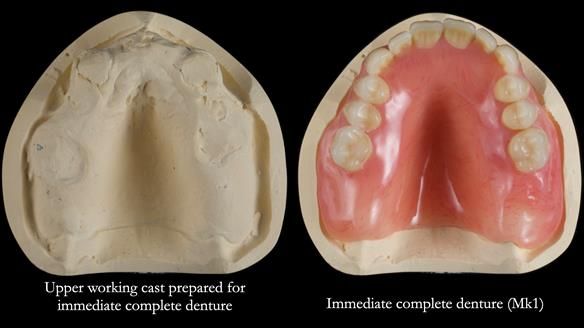
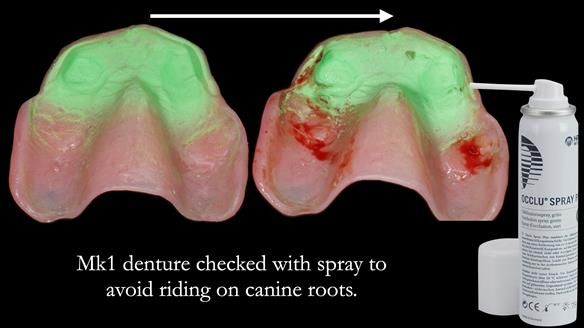
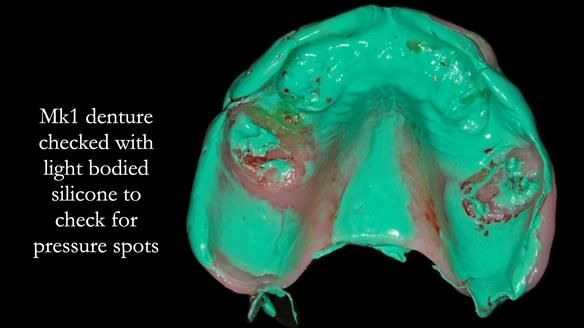
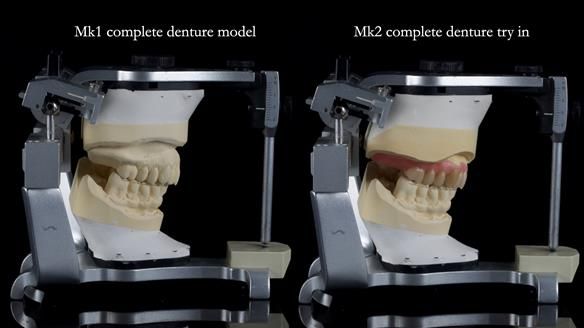
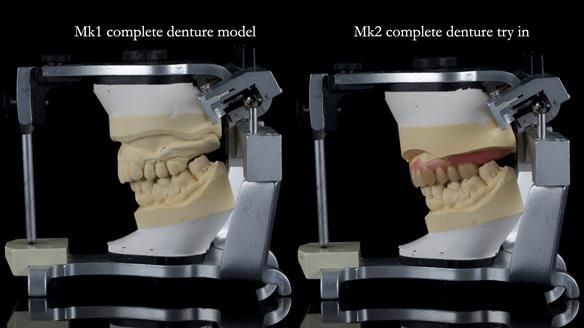
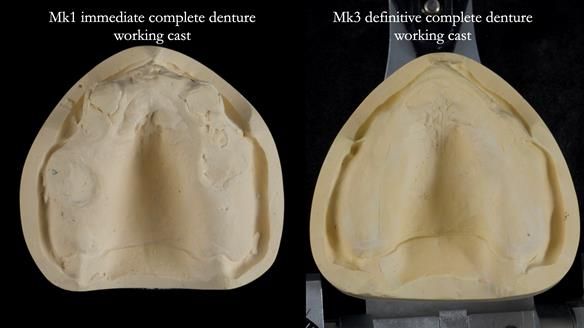
- Retain the upper canines (13 and 23) after root canal treatment, to support a Mk1 immediate complete denture.
- After 9–12 months, replace the Mk1 with a definitive Mk2 metal-based complete upper denture.
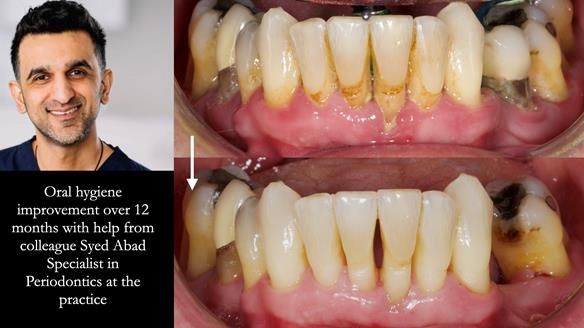
- Periodontal therapy was carried out to help maintain the lower teeth for as long as possible.
Initially, the plan was to retain the canine roots (13 and 23) under the denture after root canal treatment, as set out in the original treatment plan letter.
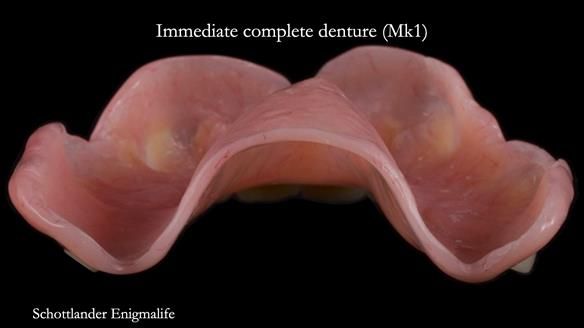
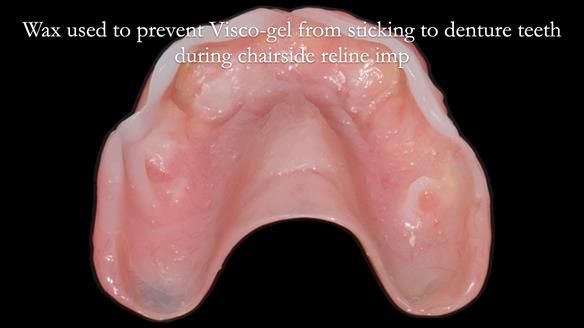
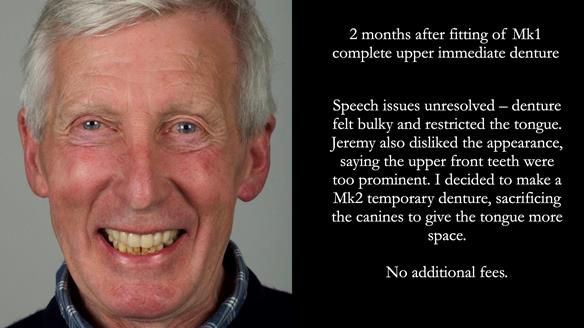
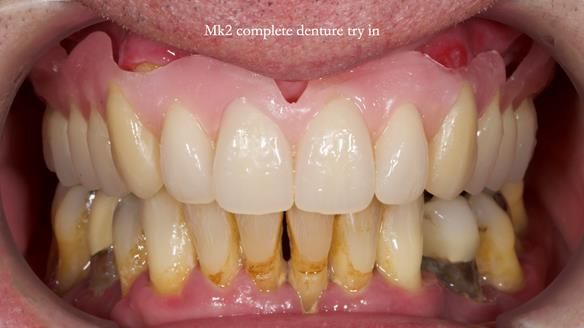
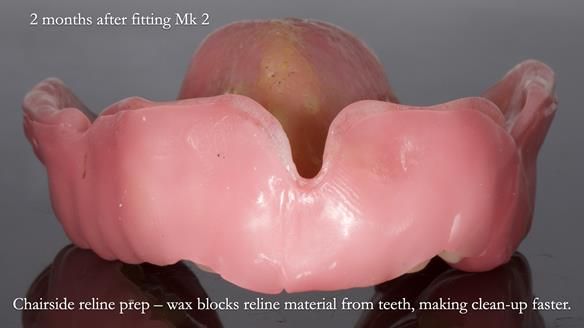
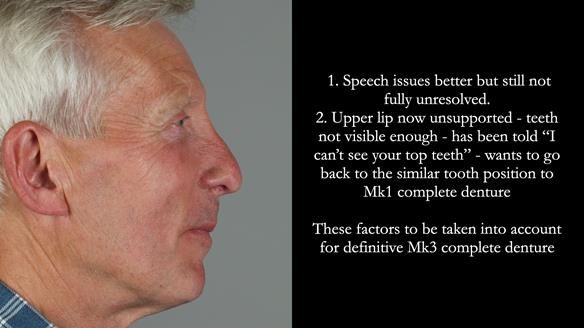
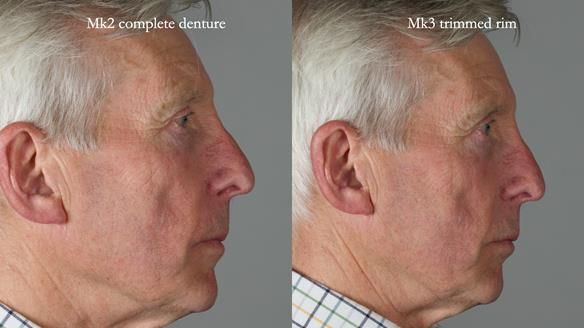
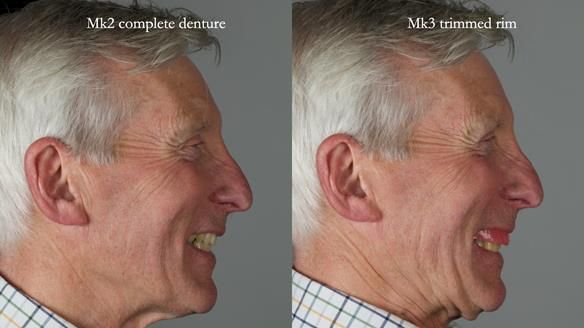
After fitting the Mk1 immediate denture, Jeremy experienced speech problems, particularly with ‘s’ sounds, and felt the denture was too bulky, restricting his tongue. Although the appearance was good, the speech issues could not be resolved.
Two months later, after careful discussion with Jeremy, I decided to revise the plan:
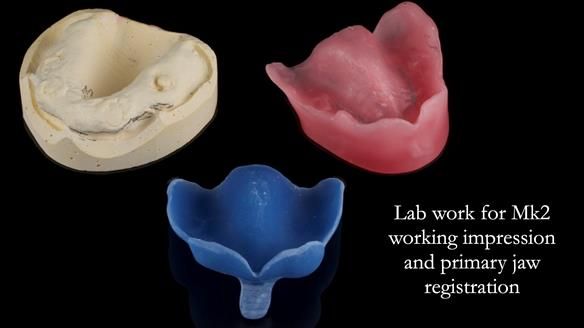
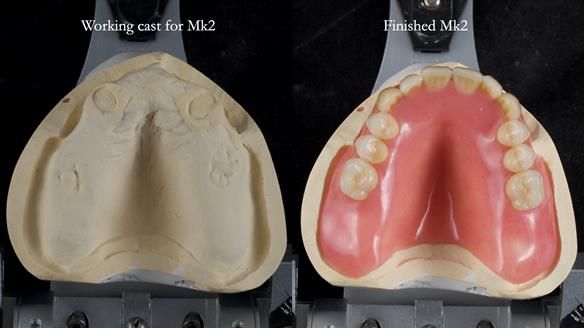
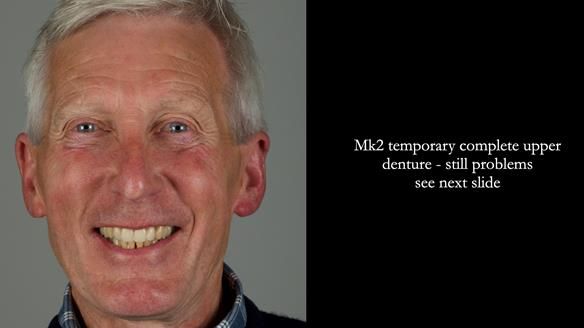
We sacrificed the upper canine roots and made a Mk2 temporary complete denture to provide more tongue space and improve speech.
This is part of the nature of providing high-quality denture care — sometimes we need to adapt the plan to achieve the best result for the patient.
Importantly, I budget for the potential need to make a Mk2 temporary denture in cases like this, so patients are not charged extra if we need to adjust the original plan.
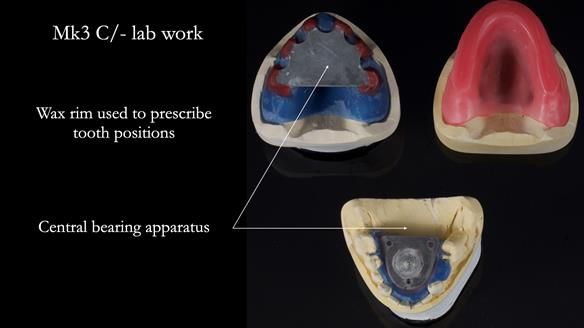
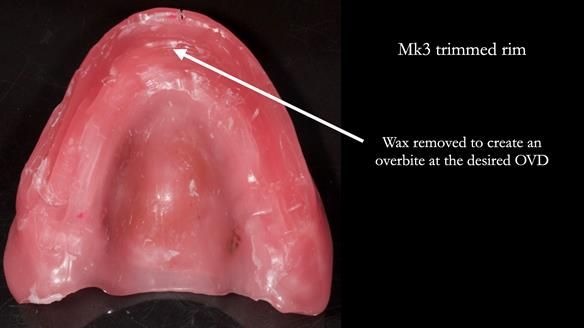
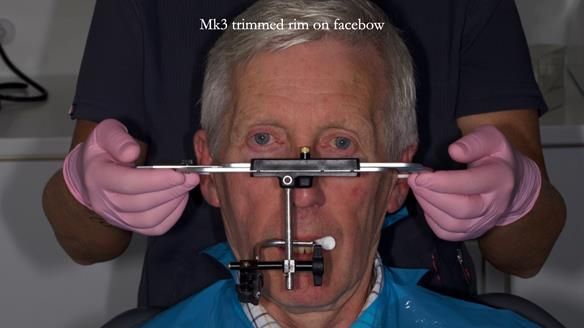
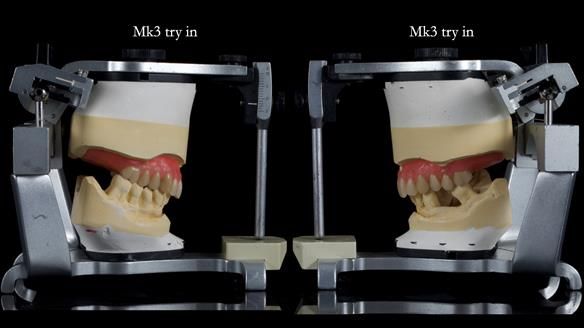
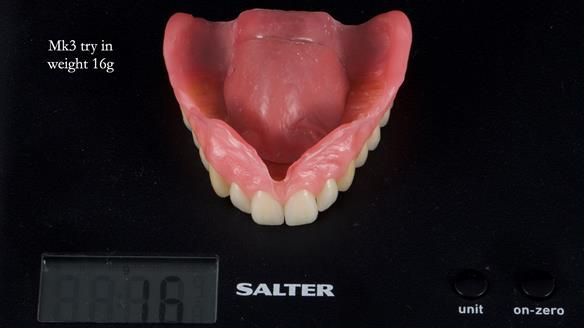
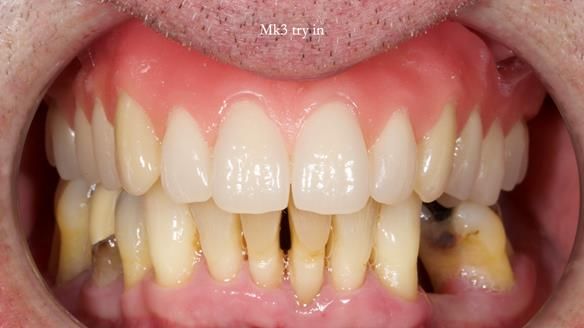
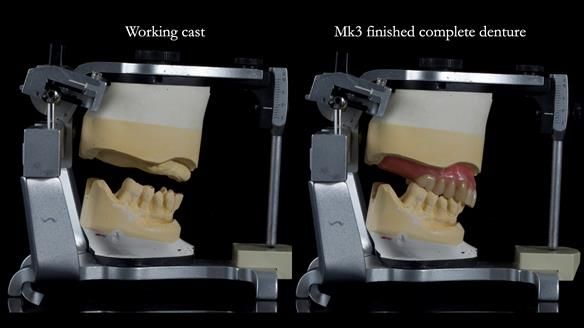
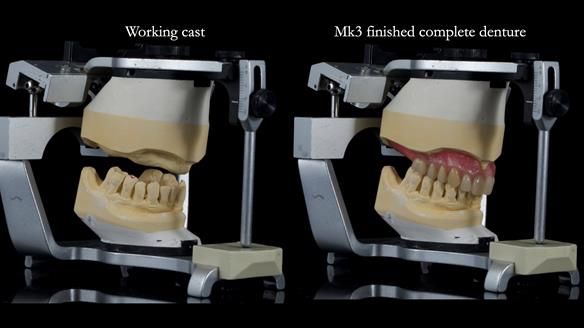
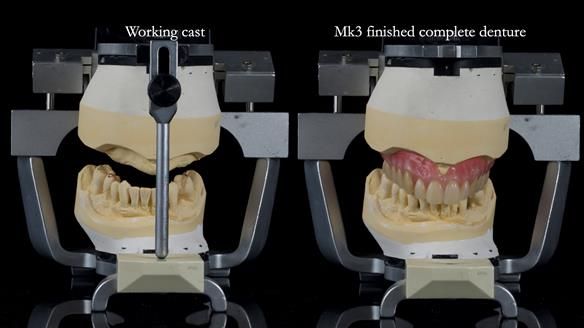
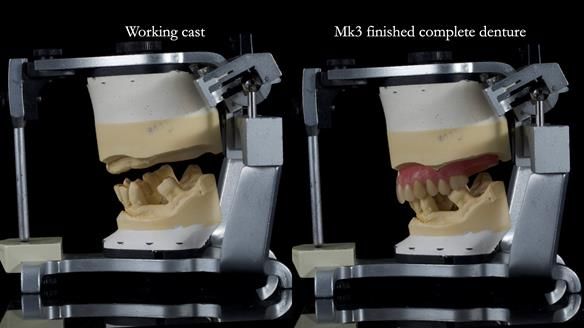
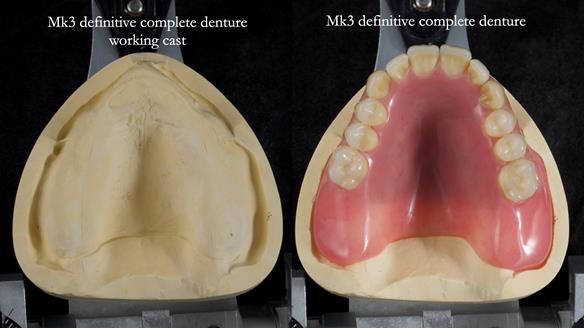
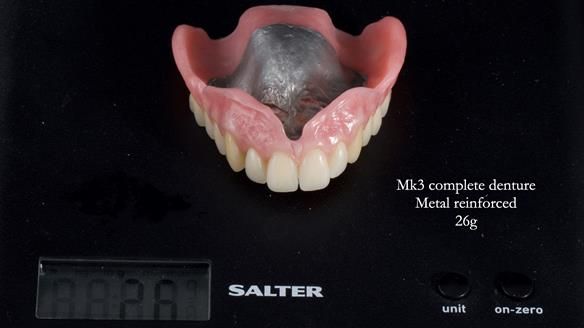
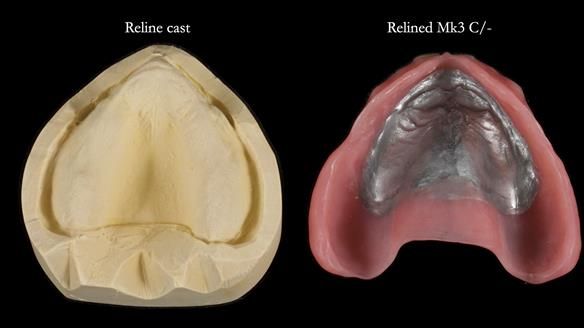
Twelve months after the final extractions, I made the Mk3 definitive complete upper denture.
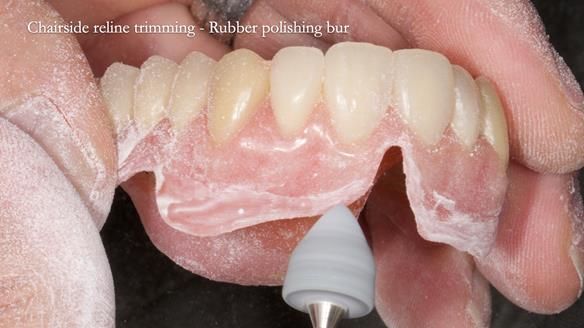
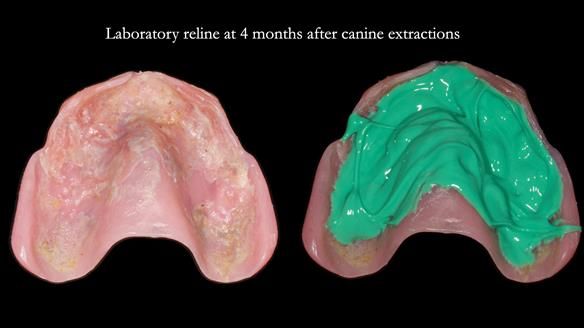
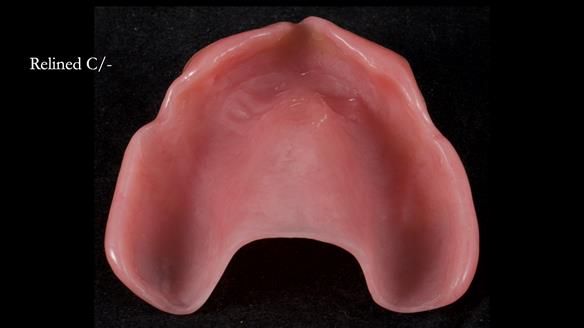
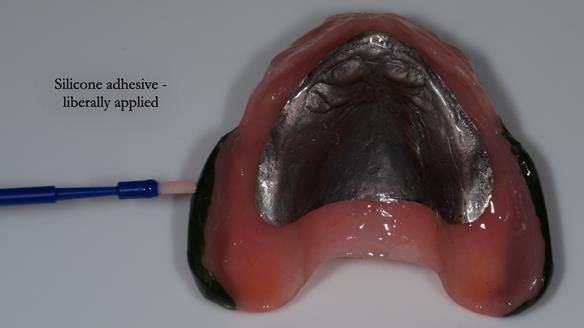
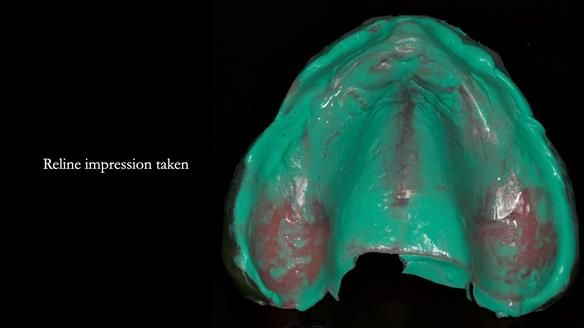
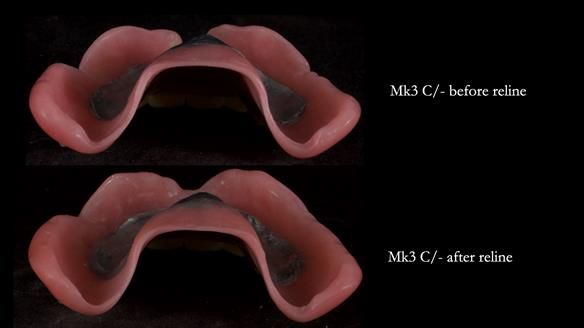
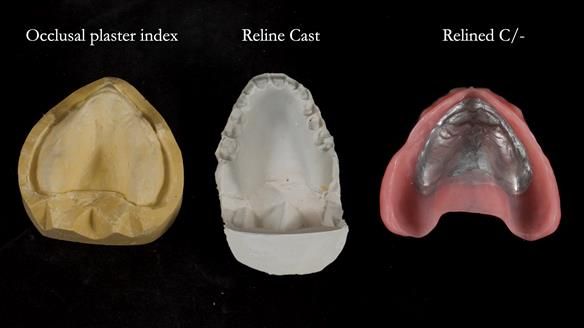
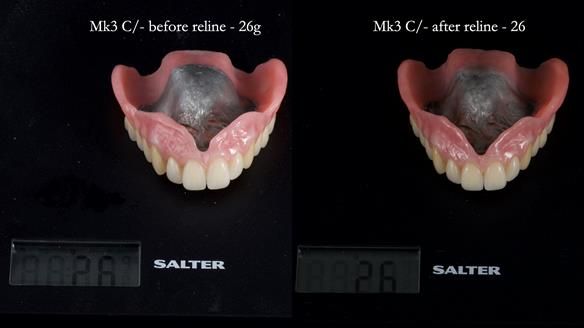
Three months after fitting, a reline was carried out to adapt to tissue changes from the canine and molar extractions.
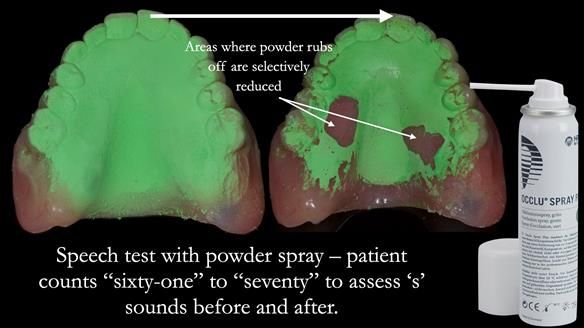
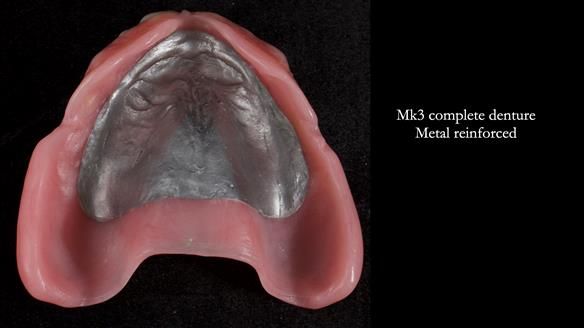
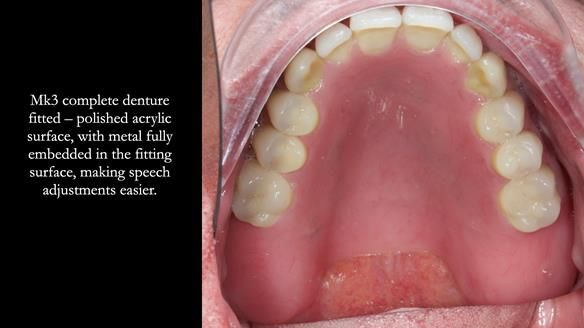
For the Mk3, we embedded the metal base fully within the fitting surface acrylic. This design allowed adjustment of the polished surface using universal marking spray to fine-tune sibilance and prevented any join between the metal and acrylic from being felt by the tongue.
This approach solved most (but not all) of the speech issues.
At Jeremy’s final review:
- Retention, stability and support were excellent.
- Speech was good but not perfect.
- Aesthetics were excellent and Jeremy was very happy with this apspect.
- Sibilance with S’s was still a bit of a problem for him, however, Claire (my nurse) and I could not hear problems with the speech.
- Biting and chewing were no problem at all.
- Amazing improvement in oral hygiene and response to Syed’s periodontal therapy.
Most importantly, Jeremy was a genuinely nice person whom I thoroughly enjoyed treating. He fully understood the limitations and worked closely with us throughout his treatment.
.........................................................................................



























































































































































































Finlay Speaking at the SWARD Annual Meeting 2026
I’m delighted to announce that I’ll be presenting at the SWARD Annual Meeting on Friday, 6th February 2026 in Dallas, Texas.
My session will focus on removable prosthodontics – a vital but often underappreciated area of dentistry. I’ll be sharing practical techniques and insights from clinical cases that span:
Complete Dentures – achieving maximum fit, function, and aesthetics
Partial Dentures – using the biologically healthy Scandinavian design system
Implant-Supported Overdentures – best practices for Locators® and bar attachments
This session is designed for the whole dental team – dentists, prosthodontists, denturists, and technicians. My goal is to share useful, actionable tips that you can take straight back to the clinic or lab.
Rowan Garstang is coming too!
I’m thrilled that Rowan, my dental technician, will be joining me in person. While he won’t be presenting, he’ll be there to answer any technical or laboratory-related questions during the day.
If you’re attending, I strongly encourage you to bring your technician along. This day is an ideal opportunity for clinicians and technicians to learn together, share perspectives, and strengthen communication.
A glimpse of the day:
Morning – Complete and Partial Dentures:
Theory + practical case demonstrations
Afternoon – Advanced Partial Dentures +
Implant-Supported Overdentures:
Design, fit, and patient-centred outcomes
Dentures remain a critical option for many patients who can’t have implants – whether due to medical reasons, cost, or personal preference. Done well, they can offer beautiful aesthetics and long-term function that often rival fixed prosthodontics.
A big thank you to the SWARD Council for the invitation.
Rowan and I are really looking forward to it!
Warm regards,
Finlay Sutton