Covid-19 and my denture courses
** I plan on running my courses on complete dentures, partial dentures, immediate dentures and implant supported overdentures as soon as it is safe to do so. I will keep you up dated via Newsletters and my website. **
In the mean time I have been providing individual coaching, mentoring and treatment planning for removable prosthdontics via private recorded zoom meetings. They have been a great success with dentists all over the world taking part. The sessions are recorded so the mentee can refer back to the sessions. These can be one off or multiple sessions. Please click here for further information.
Finlay's Case Presentation
Welcome to my August 2020 Newsletter Case Presentation
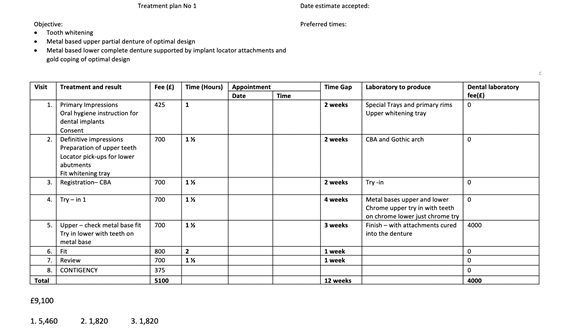
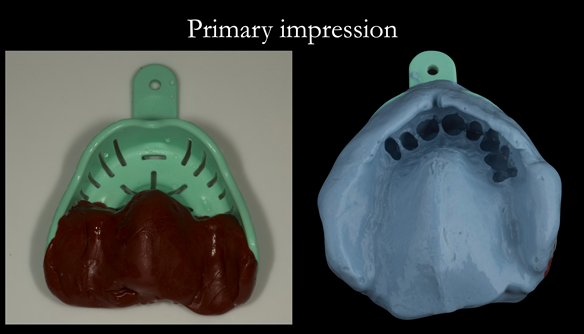
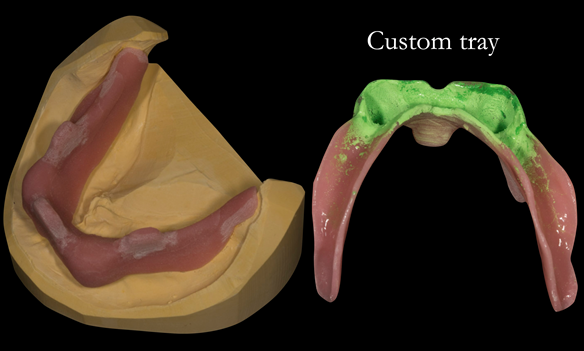
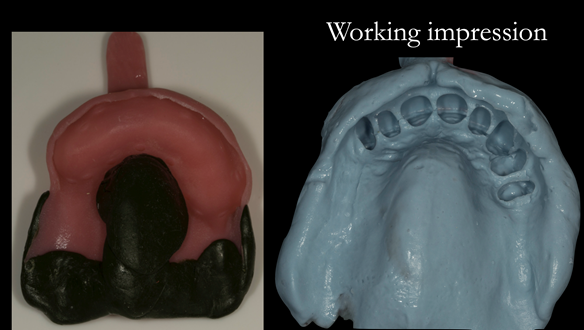
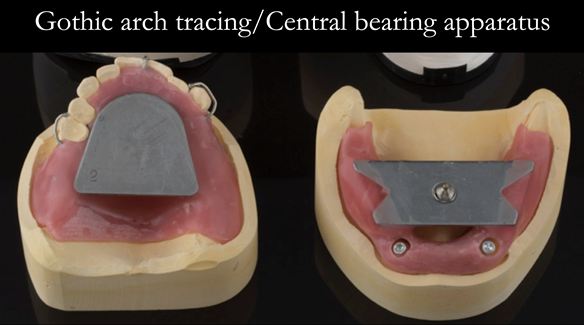
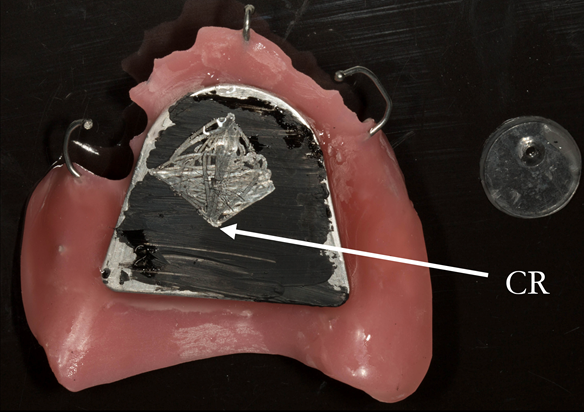
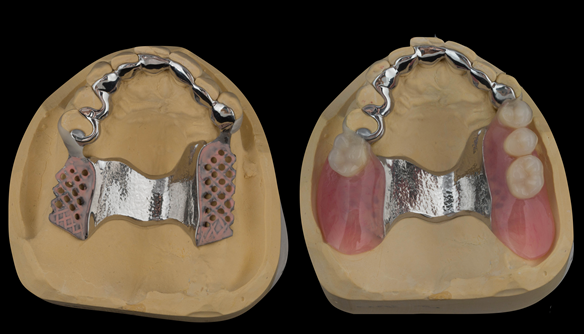
This newsletter describes in step by step detail the provision of an upper free end saddle partial denture in a patient with a high smile line and lower implant supported complete denture with suboptimal positioned dental implants.
This 75 year old woman was referred to me from her general dental practiioner.
Dental History and Concerns
An implant supported lower complete lower denture had been provided 4 years previously in the UK. This "no longer fixes to its anchors and is worn". The upper partial denture was over 12 years old, having been provided in the USA. “Upper partial again worn and a little unreliable.”
Social History
Nil.
Dental wish list
“Good eating teeth – and ones/teeth that I am happy to smile with.”
Diagnoses
- The remaining natural upper 8 teeth had reduced but healthy periodontal attachment.
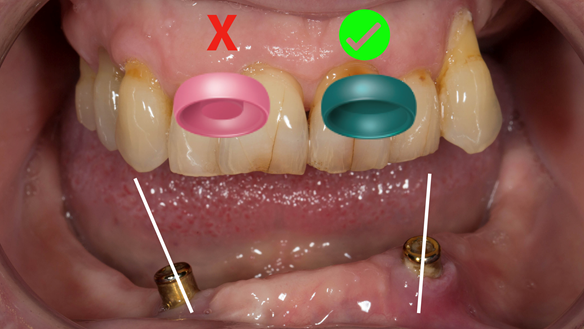
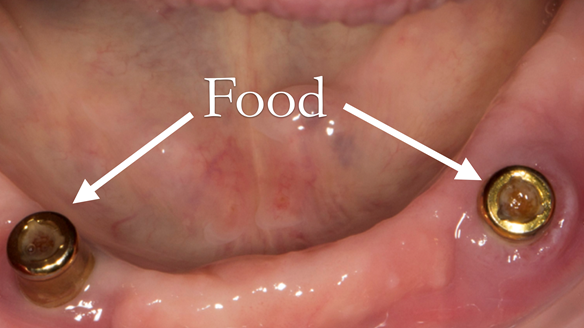
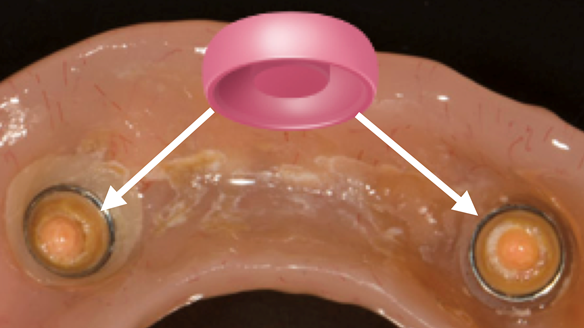
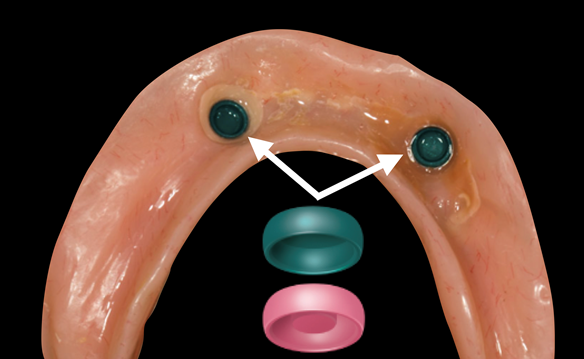
- The two dental implants (Astra) in the lower jaw had Locator attachments and appeared healthy. The implants positions were suboptimally positioned being over 30 degress divergant, resulting in poor fixation and increased wear of the Locator components.
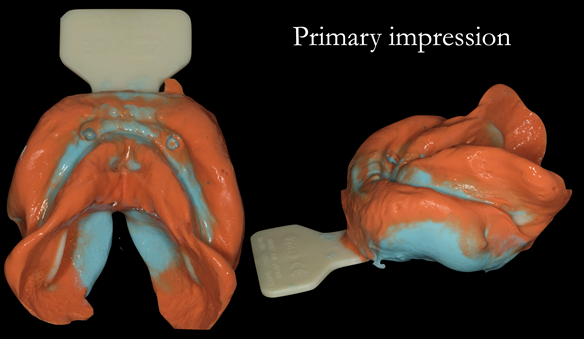
- The upper and lower dentures exhibited suboptimal extension of the flanges and saddles. They had poor retention, support and stability.
- The patient had a high smile line showing the cobablt chromium clasps of the UR4 and UL3 during social interaction.
Apart from providing no treatment we discussed two solutions namely; fixed implant supported teeth versus optimally designed and made removable dentures. The patient chose to have removable partial dentures.
The clinical situation and treatment process is shown in detail below with photographs. I provided the clinical work and Rowan Garstang provided the technical work.
If you enjoy my Newsletters and you have friends, colleagues, dental students, dental technicians, clinical dental technicians and postgraduate dentists that you think will appreciate them, please feel free to share them. In addition, if your colleagues would like to receive our Newsletters please email me and I will add them to my email list.





















Reference material
Full access PDF to my published scientific papers which explain my philosophy and clinical techniques. Please click on the link below and scoll down this page to find lots of useful clinical techniques, reference material and previous lectures:
https://www.finlaysutton.co.uk/speaking